External Contribution: Diana Rayes, Program Director for the Faith and Global Health Initiative at Georgetown University’s Global Health Institute
- Issue 13
 Diana Rayes, Program Director for the Faith and Global Health Initiative at Georgetown University’s Global Health Institute
Diana Rayes, Program Director for the Faith and Global Health Initiative at Georgetown University’s Global Health Institute
 Diana Rayes, Program Director for the Faith and Global Health Initiative at Georgetown University’s Global Health Institute
Diana Rayes, Program Director for the Faith and Global Health Initiative at Georgetown University’s Global Health InstituteFourteen years of conflict left Syria facing one of the world’s most protracted humanitarian crises. The fall of the Assad regime in December 2024 created a new political reality—and a brief window for the transitional government led by Ahmad al-Sharaa to rebuild the country’s shattered health system. Yet despite new leadership and international partnerships, the fundamentals remain unchanged: immense need, destroyed infrastructure, a depleted workforce, and a deep financing gap
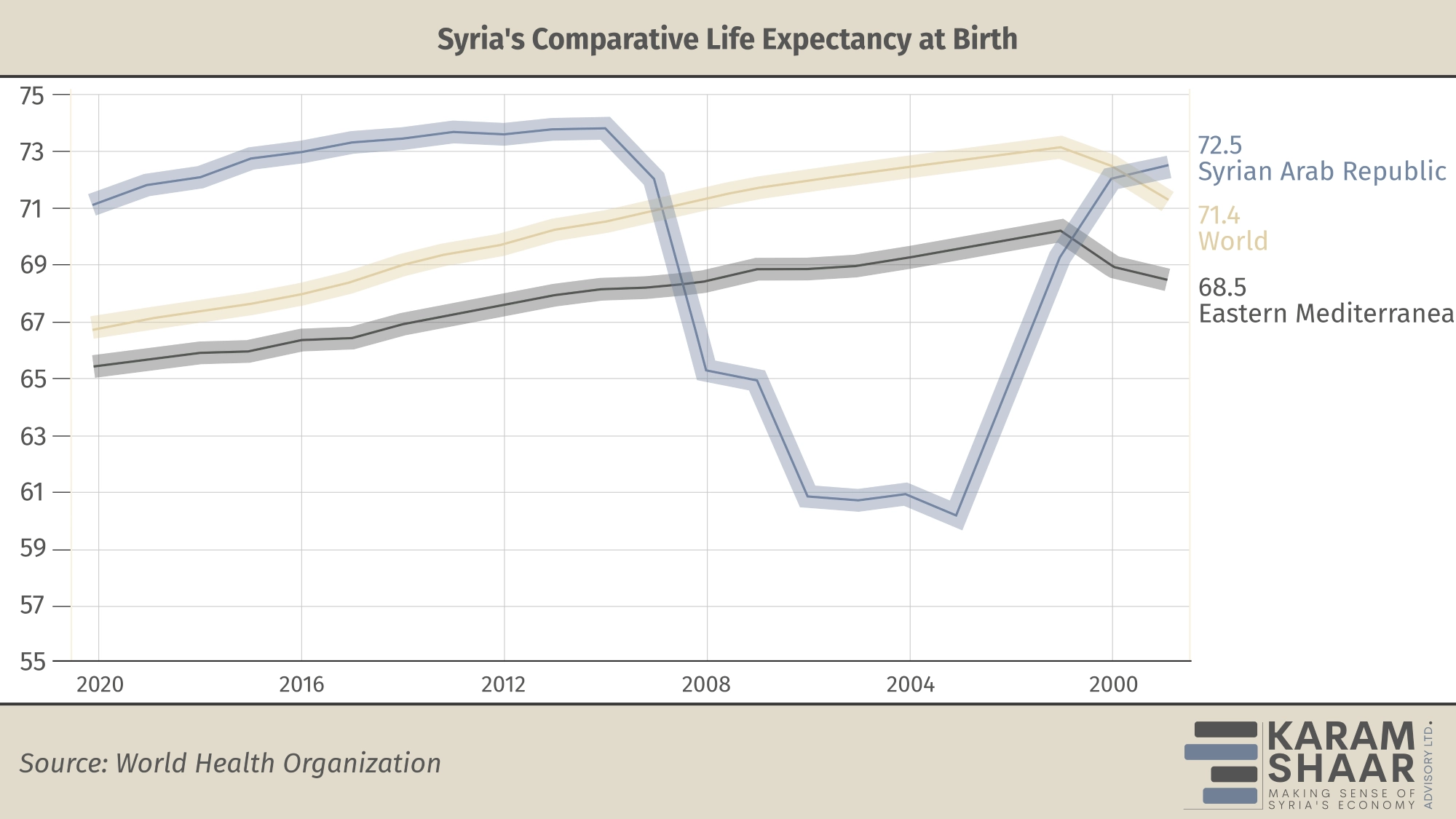
Nearly 16.5 million Syrians—over 70 percent of the population—depend on humanitarian assistance, and 15.9 million require health services. Poverty drives deep health inequality, with an estimated 90 percent of Syrians living below the poverty line and many forced to choose between food, electricity, or medical care. Life expectancy stood at 72 years before the conflict and dropped to a low of 60 in 2017—a 12-year decline in less than a decade. Chronic diseases remain leading causes of death, yet prevention and treatment services are extremely limited. Without reforms that restore access, affordability, and trust, recovery will remain out of reach for most Syrians.
A Fragmented System
The conflict left Syria’s health system deeply fragmented, marked by three distinct governance models that emerged during the war: areas once controlled by the regime, the northwest (under Hay’at Tahrir al-Sham), and the northeast (under the Autonomous Administration of North and East Syria, or Rojava).
The legacies of these parallel systems still hinder coordination and continuity of care. The effects are most evident in rural and underserved areas, where recurring waterborne disease outbreaks, landmine injuries, and critical gaps in maternal, mental, and noncommunicable disease care persist. Noncommunicable diseases account for over 70 percent of all deaths in Syria, yet facilities offering essential drugs and treatment options remain scarce.
Tackling this fragmentation was among the first challenges for interim Health Minister Dr. Musaab Nazzal al-Ali, a neurosurgeon appointed in March 2025 after Dr. Maher al-Sharaa, the interim president’s brother, briefly held the post. Despite genuine efforts to reorganize the system, humanitarian priorities—especially the vast destruction of healthcare facilities—still dominate, overshadowing long-term recovery and institution-building.
Extent of Destruction
The destruction of Syria’s health system remains vast. The World Health Organization (WHO) estimates that 38 percent of hospitals and 59 percent of primary health facilities were partially or completely nonfunctional after the conflict. In research conducted with colleagues at Johns Hopkins, UC Berkeley, and the Syrian American Medical Society, we found that attacks on healthcare compounded effects—destroying infrastructure, eroding trust, deterring patients from care, and forcing health workers into impossible ethical choices.
Attacks on healthcare—including medical facilities, ambulances, and health workers—continue inside Syria, with over 30 incidents in 2025, including the deaths of at least five healthcare workers. Although this marks a decline from 62 attacks in 2024, several occurred in As-Suwayda, which saw a surge of violence in July 2025 that triggered an ongoing humanitarian emergency. The interim government’s response has underscored the deep trust deficit between state institutions—especially the Ministry of Health—and Syria’s minorities.
“Re-establishing legitimacy is a critical entry point for rebuilding the health system in Syria,” says Dr. Munzer Alkhalil, chair of the Syria Public Health Network. “One key piece is adopting a hybrid governance model and avoiding an extreme top-down or bottom-up governance approach.”
Alkhalil, formerly director of the Idlib Health Directorate, says the experience of an independent health system in northwest Syria offers key lessons on how governance endured despite the absence of a functioning state. His core message is that health must be treated as a shared civic endeavor rather than a political tool—balancing supply and demand while empowering both central and local authorities to restore the system’s functionality and credibility.
The Health Workforce Challenge
The exodus of health workers remains one of the greatest barriers to recovery. An estimated 70–80 percent of doctors and nurses have left the country, leaving hospitals short of staff, supplies, and equipment. Many of Syria’s most qualified physicians, nurses, and specialists now live abroad—in Egypt, Türkiye, Germany, and the UK. Through the Syria Public Health Network, we studied this displaced workforce and found that professionals face major challenges adapting their degrees and integrating into host-country health systems, underscoring the need for substantial incentives to support their reintegration.
This is a monumental task for the Ministry of Health. A review I led for the Lancet–AUB Commission on Syria found that few post-conflict settings have successfully implemented programs to bring health professionals home. In Afghanistan and Cambodia, early workforce assessments helped identify capacity and design targeted incentives. To my knowledge, Syria has yet to conduct a similar mapping exercise.
Rebuilding the health system should therefore be seen not only as a development goal but as a prerequisite for the return and reintegration of Syria’s health workforce. Without functioning institutions, displaced professionals will remain abroad, and Syrians at home will continue to face severe gaps in care.
Syria’s Transitional Phase
Syria now stands in a fragile “transitional phase,” the uncertain period between the end of conflict and the start of reconstruction, when the interim government and emergency health providers must work in tandem. Its immediate challenge is to meet urgent health needs while laying the foundation for a sustainable, nationally led system that can endure beyond humanitarian relief.
Other post-conflict countries have faced similar challenges of fragmentation, displacement, and donor dependency, offering lessons for Syria. A key takeaway is that successful transitions require clear national strategies aligning humanitarian aid with state-building goals.
But Syria’s case is atypical. The Ministry of Health was reconstituted relatively quickly under the transitional government, and early agreements with NGOs and UN agencies such as the WHO sought to stabilize service delivery. On its official website, the Ministry outlines a vision to improve population health, strengthen key indicators, and promote equity through cross-sectoral collaboration. Yet no comprehensive national health plan has been enacted. Progress remains limited to piecemeal decrees and ministerial decisions on appointments and the distribution of medical supplies.
The key question now is whether this vision can evolve into a unified national system that addresses chronic and preventive care beyond emergency response. For Syria, this means: managing international stakeholders through transparent, results-based partnerships; avoiding donor-driven fragmentation by developing a single, nationally led health strategy; balancing investment across all six WHO health system building blocks rather than focusing solely on physical reconstruction; and preventing a two-tiered system where NGO services operate apart from those of the Ministry.
This transitional moment should be seen not as a pause between crisis and reconstruction, but as the decisive phase of recovery—one that will determine whether Syria’s future health system becomes more equitable and cohesive than ever before.
The Funding Gap
Syria’s health reconstruction will shape not only national recovery but regional stability. Yet the financing outlook remains dire: just seven percent of the USD 566 million needed for the humanitarian health response has been secured—covering only immediate needs, not the billions required for long-term rebuilding.
Restoring Syria’s health system will demand major investment in infrastructure, supply chains, workforce training, digital information systems, and specialized care. The WHO recommends that 15 percent of national budgets go to health—a target Syria remains far from meeting.
A Shifting Donor Landscape
Syria’s health recovery faces growing pressure from changing donor priorities at home and abroad. The US—historically the largest humanitarian donor—has reduced funding, causing the closure of more than 150 health facilities and affecting 4.4 million people across nine governorates. These cuts come at a critical point in Syria’s fragile recovery.
European and regional donors have maintained or slightly increased support, though often through narrow or inflexible partnerships. What Syria needs now is not another round of short-term appeals, but a shift toward multi-year, development-oriented funding that builds institutions rather than sustains emergency care. Encouragingly, new health partnerships with Gulf countries such as Saudi Arabia and Qatar suggest this transition is possible.
The Syrian diaspora—particularly its large community of health professionals—remains an untapped asset. Policies promoting remote engagement, mentorship, and short-term missions could link local needs with global expertise. The Ministry has shown openness to diaspora and international support, but coordination would improve through a dedicated focal point within the Ministry to manage these relationships.
The Road Ahead
Post-conflict recovery is never straightforward, and the first few years often determine whether institutions take hold or falter. Syria’s interim authorities—working with dedicated technocrats and health professionals—now stand at a pivotal crossroads for rebuilding the nation’s health system.
Experience from other post-conflict settings shows that early investments in health are both a social imperative and a foundation for rebuilding trust, legitimacy, and stability. Strong health systems reduce mortality and morbidity while restoring the social contract between citizens and the state—absent in Syria for over five decades under Assad rule.
If donors align with national priorities, the diaspora’s expertise is mobilized, and reconstruction is guided by equity and accountability, Syria could emerge with a stronger, more resilient health system. As the World Bank’s Toll of War report noted in 2017, more Syrians may have died from the collapse of the health system than from direct violence—a reminder that health recovery is not peripheral to peacebuilding but central to it.